If reflux symptoms persist over a prolonged period or recur after discontinuation of medical therapy, a structured diagnostic evaluation is recommended.
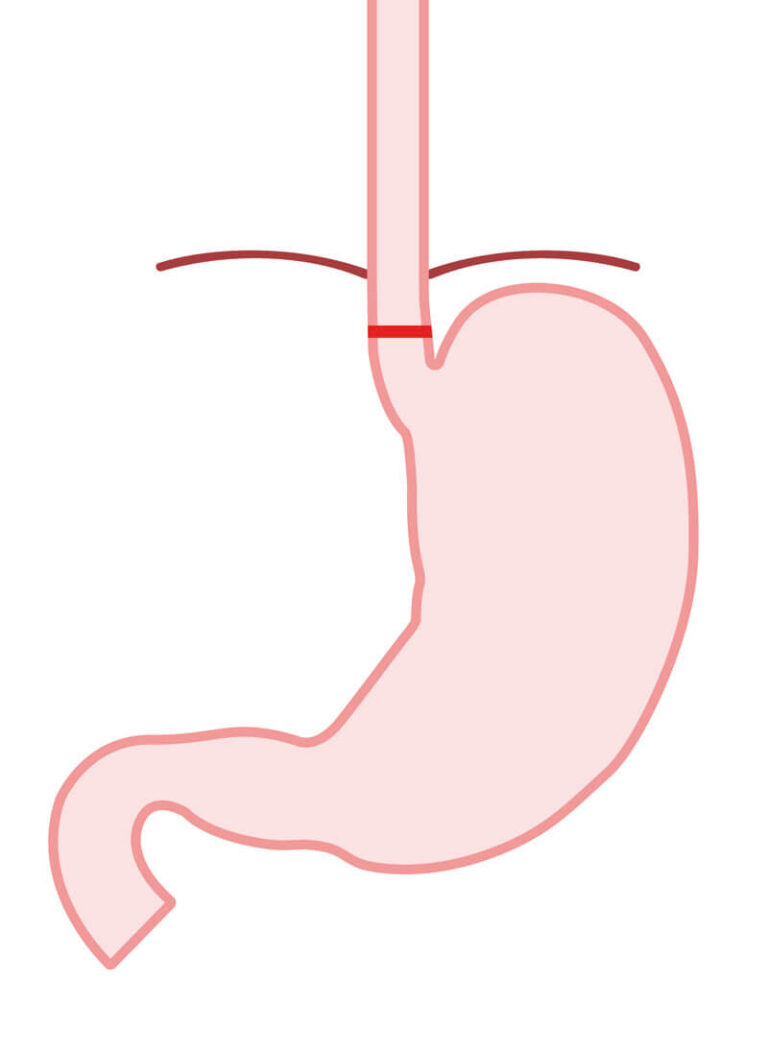
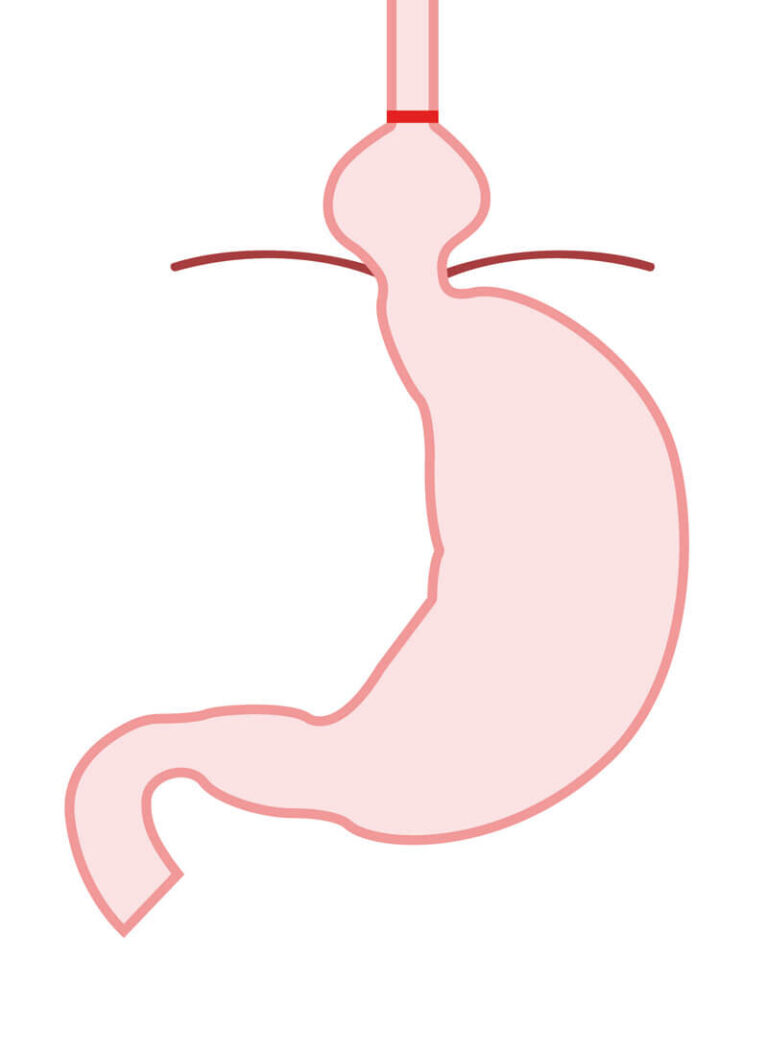
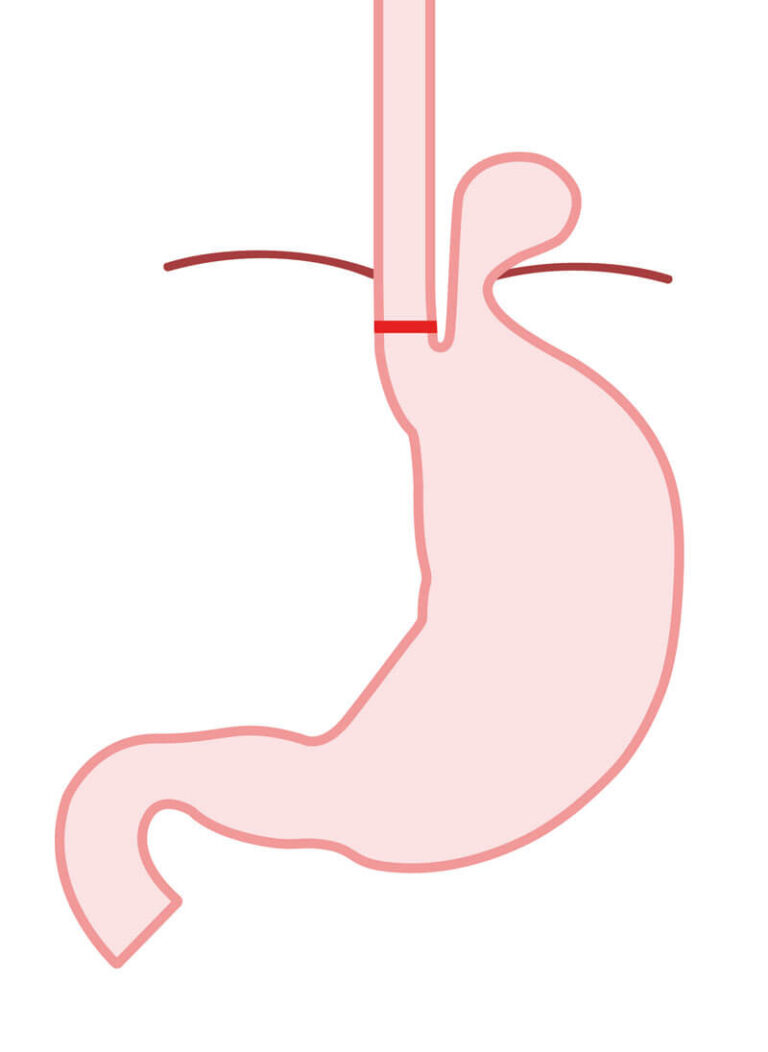
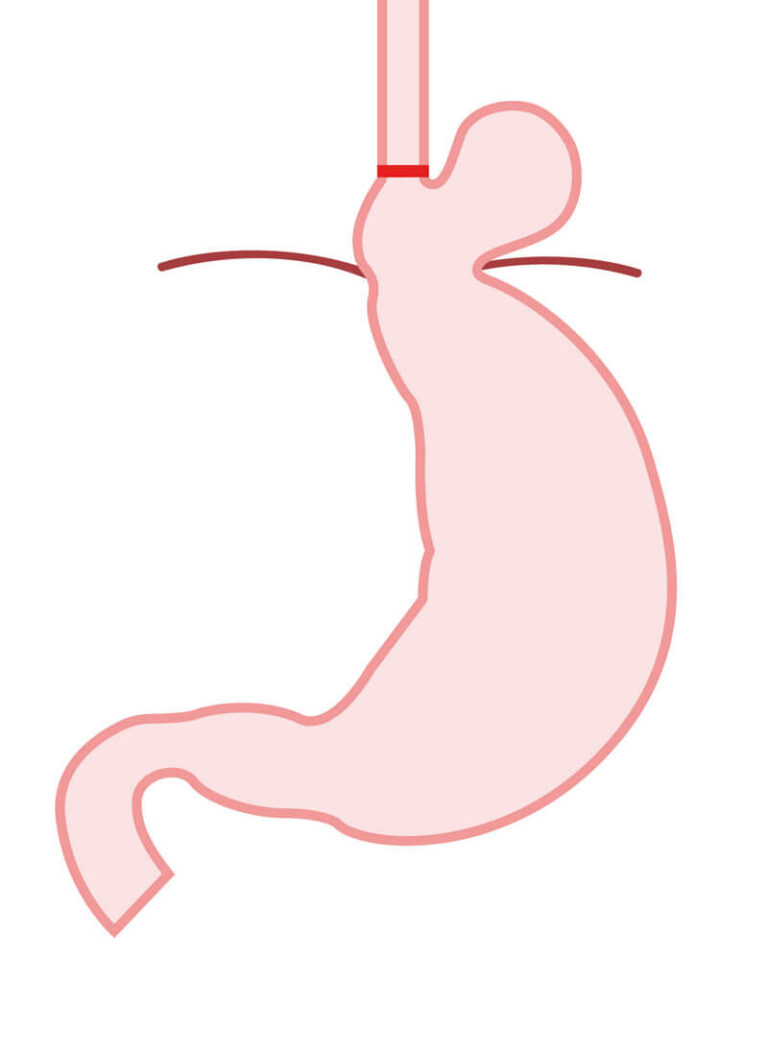
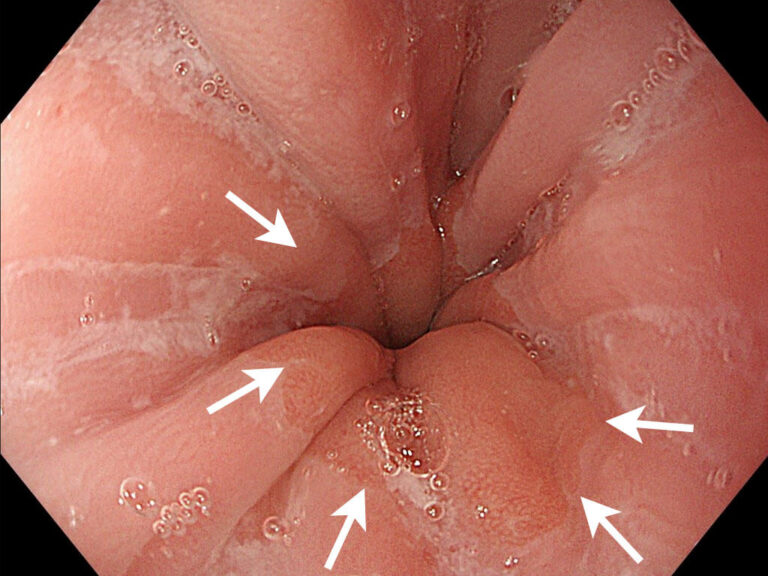
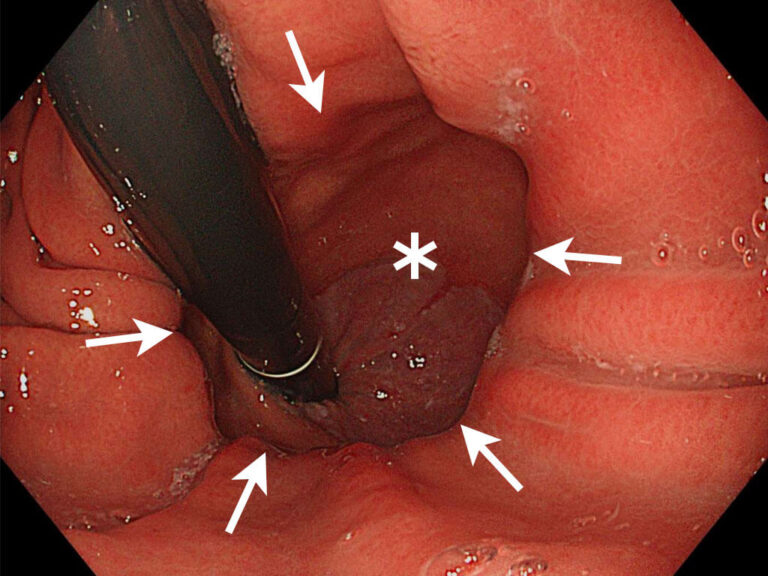
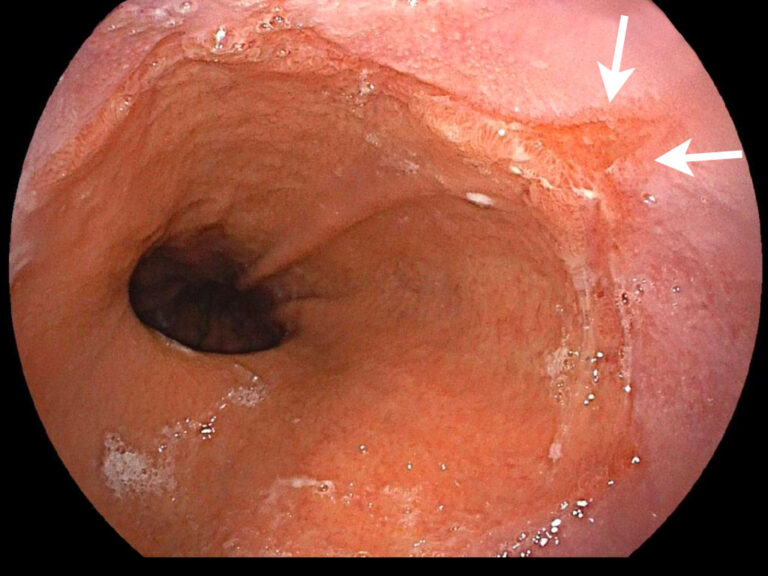
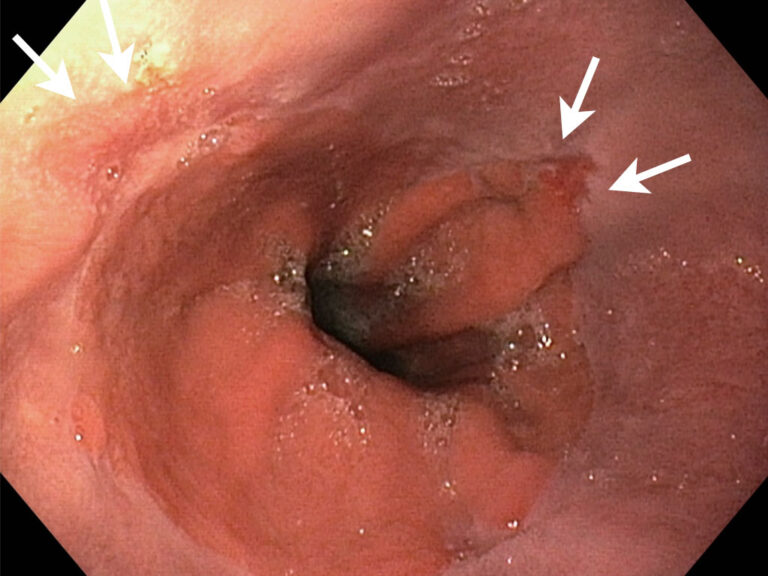
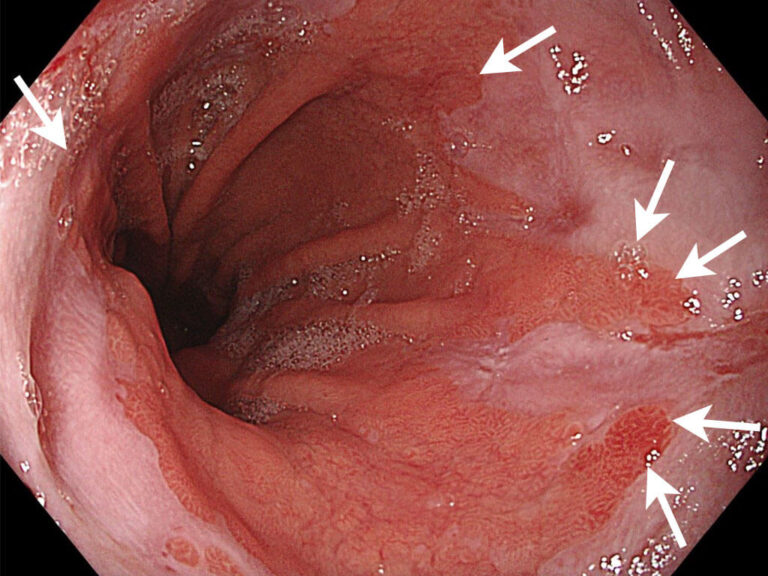
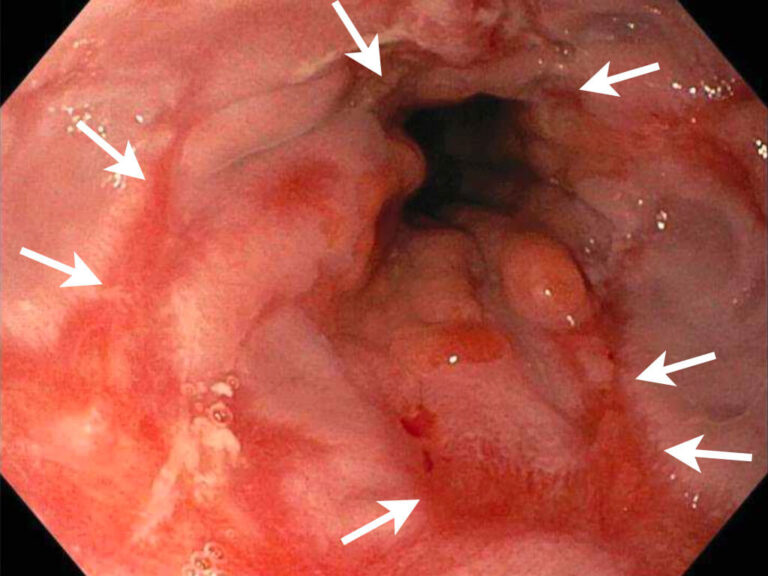
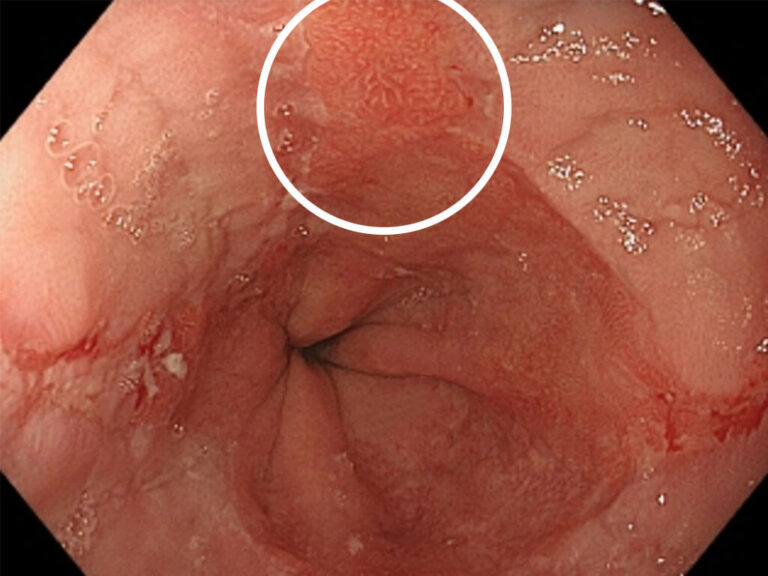
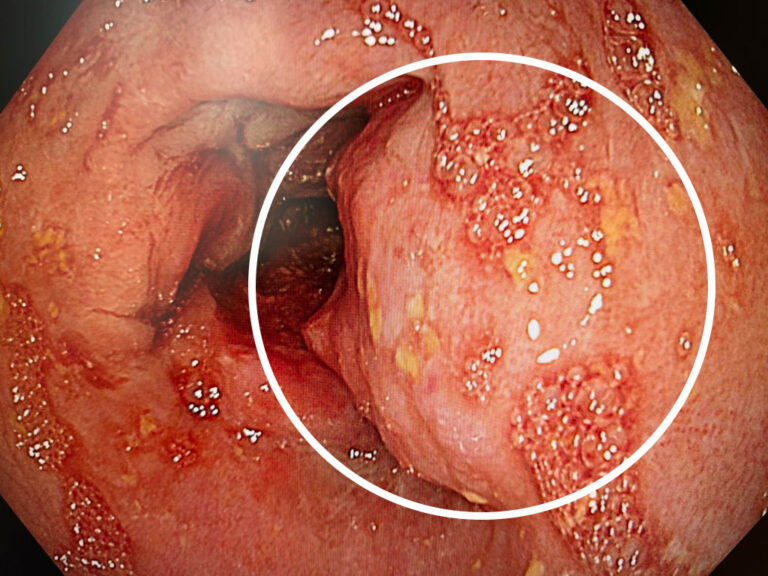
Upper endoscopy (gastroscopy) is central to the diagnostic evaluation. This allows direct assessment of inflammatory changes, Barrett’s mucosa, and the presence of a hiatal hernia. If indicated, tissue samples (biopsies) are obtained to allow for a more detailed evaluation of the mucosa.
For a functional assessment of the junction between the esophagus and the stomach, as well as the esophagus as a whole, additional testing may be required depending on the clinical situation.
A key role may be played by 24-hour esophageal pH monitoring. Using a thin catheter, acid exposure within the esophagus is measured. Alternatively, prolonged monitoring over 48 hours can be performed using a small capsule (e.g., Bravo Capsule). This allows objective quantification of the frequency, duration, and extent of acid reflux.
If necessary, esophageal manometry is performed. This test measures esophageal motility and coordination and is particularly important prior to surgical treatment, as impaired function must be taken into account when selecting the appropriate surgical approach.
In selected cases, additional radiologic evaluation of the esophagus with contrast medium may be performed. This allows assessment of swallowing dynamics, esophageal function, and the passage of contrast into the stomach and upper small intestine.
If required, the examination may be supplemented with solid food (e.g., bread or rusks) in order to assess function under more physiologic, real-life conditions.
This is particularly helpful in cases with inconclusive findings, complex clinical situations, or after previous surgery, providing additional important diagnostic information.
These diagnostic tests enable an objective assessment of reflux disease and form the basis for an individualized treatment strategy.